On this page: Overview | Health Planning Region | Carbapenemase-producing Carbapenem-resistant Enterobacterales (CP-CRE) | Carbapenemase-producing Carbapenem-resistant Pseudomonas aeruginosa (CP-CRPA) | Carbapenemase-producing Carbapenem-resistant Acinetobacter baumannii (CP-CRAB) | Laboratory Submissions | Additional Information
The HAI/AR Program produces quarterly case reports to inform prevention responses to help contain the spread of these highly-resistant organisms.
Organisms that have developed resistance to carbapenems are known as carbapenem-resistant organisms (CRO). Carbapenems are a class of broad-spectrum antibiotics reserved to treat serious multidrug-resistant infections. The CDC considers CROs an urgent threat in the United States. CROs are classified into two categories based on their ability to produce carbapenemases. Organisms that contain a carbapenemase are known as carbapenemase-producing organisms (CPOs). Carbapenemases are enzymes that break apart the carbapenem antibiotic, rendering it inactive and useless to treat infections. Carbapenemases are often located on mobile genetic elements (e.g., plasmids) enhancing wider spread and transmission to other patients.
Carbapenemase-producing organisms (CPOs) were added to the reportable disease list and conditions reportable by directors of laboratories on November 14, 2018. For more details for data and methods used, please see additional information section.
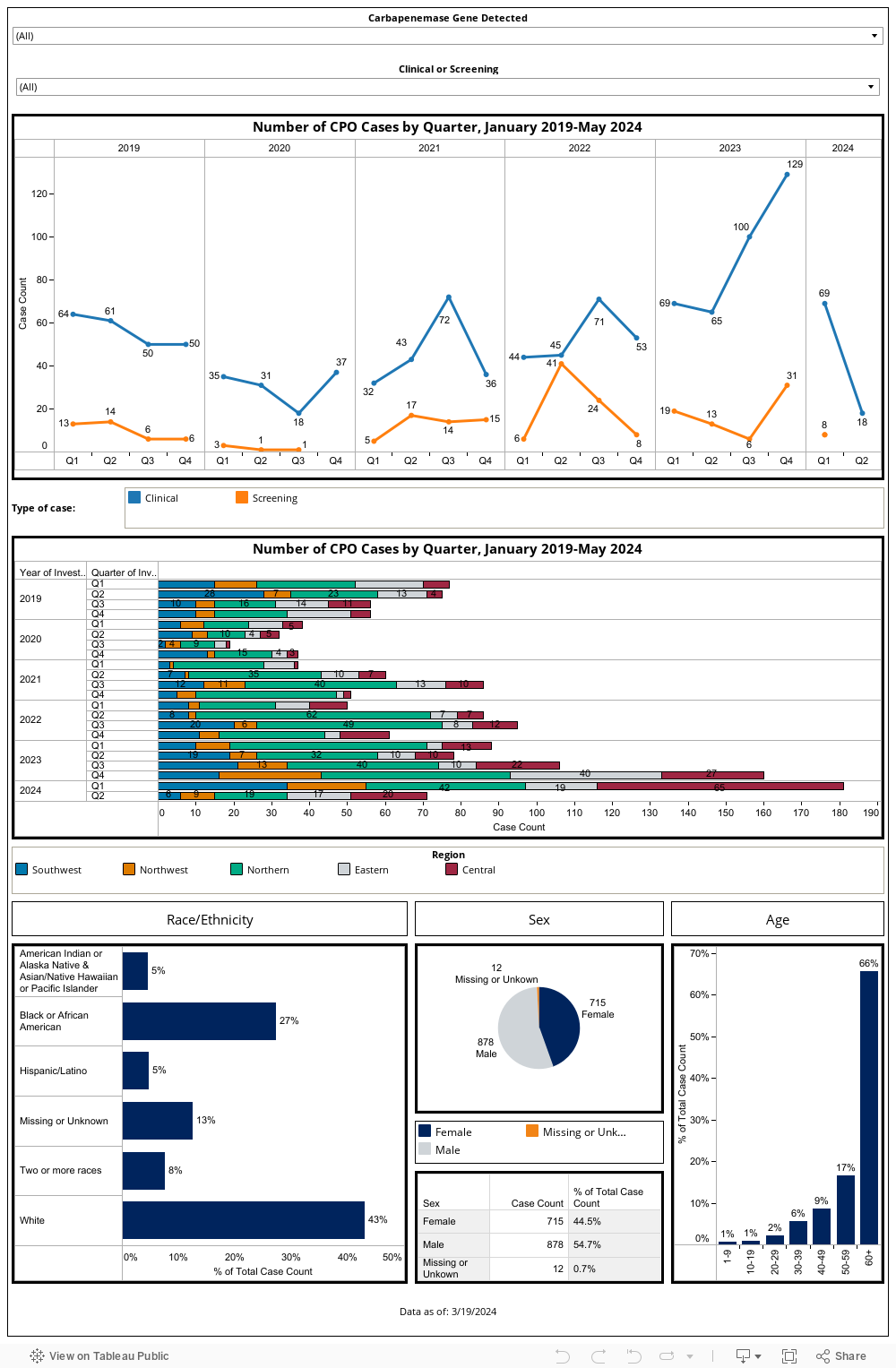
CPO Quarterly Report for Healthcare Providers Overview
Directions: Please use the filters at the top to view the data by carbapenemase genes and specimen collection reason; multiple criteria could be selected for each category.
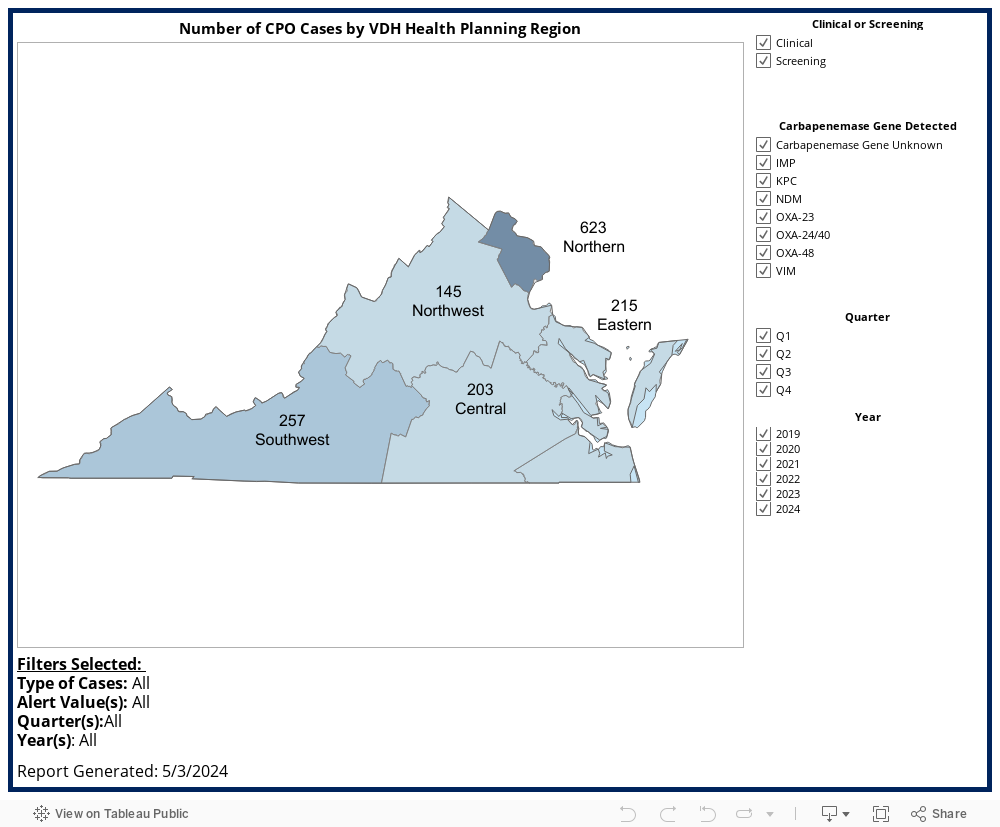
Number of CPO Cases by Health Planning Region
Directions: Please select the criteria on the right; multiple criteria could be selected for each category.
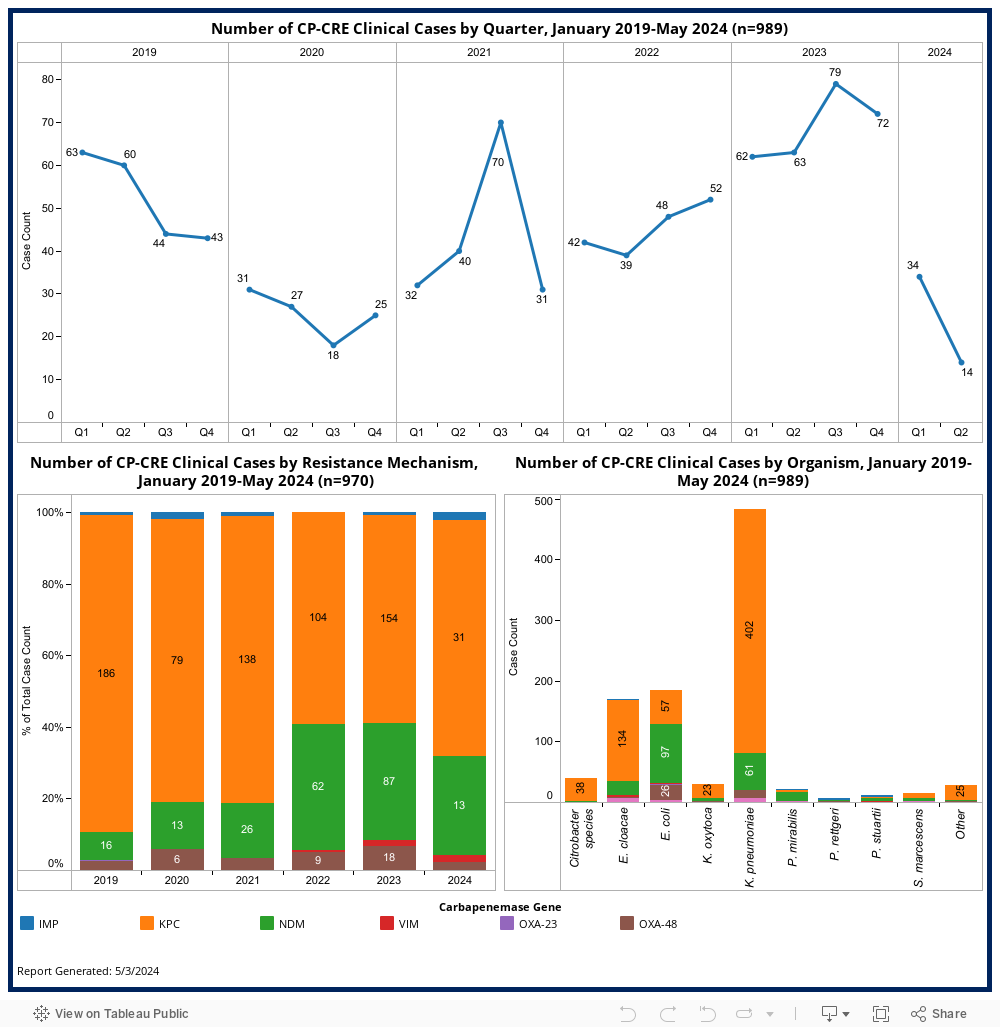
Carbapenemase-producing Carbapenem-resistant Enterobacterales (CP-CRE)
Bacteria from the Enterobacterales family, including Klebsiella species and Escherichia coli, can produce carbapenemase. According to the CDC’s AR Lab Network, about 40% of carbapenem-resistant Enterobacterales (CRE) isolates from the Mid-Atlantic region produced one of the five targeted carbapenemase genes. In addition to CP-CREs being reportable, laboratories are also required to forward CRE isolates to the state public health lab where additional testing is performed to determine the presence of a carbapenemase and the specific gene target.
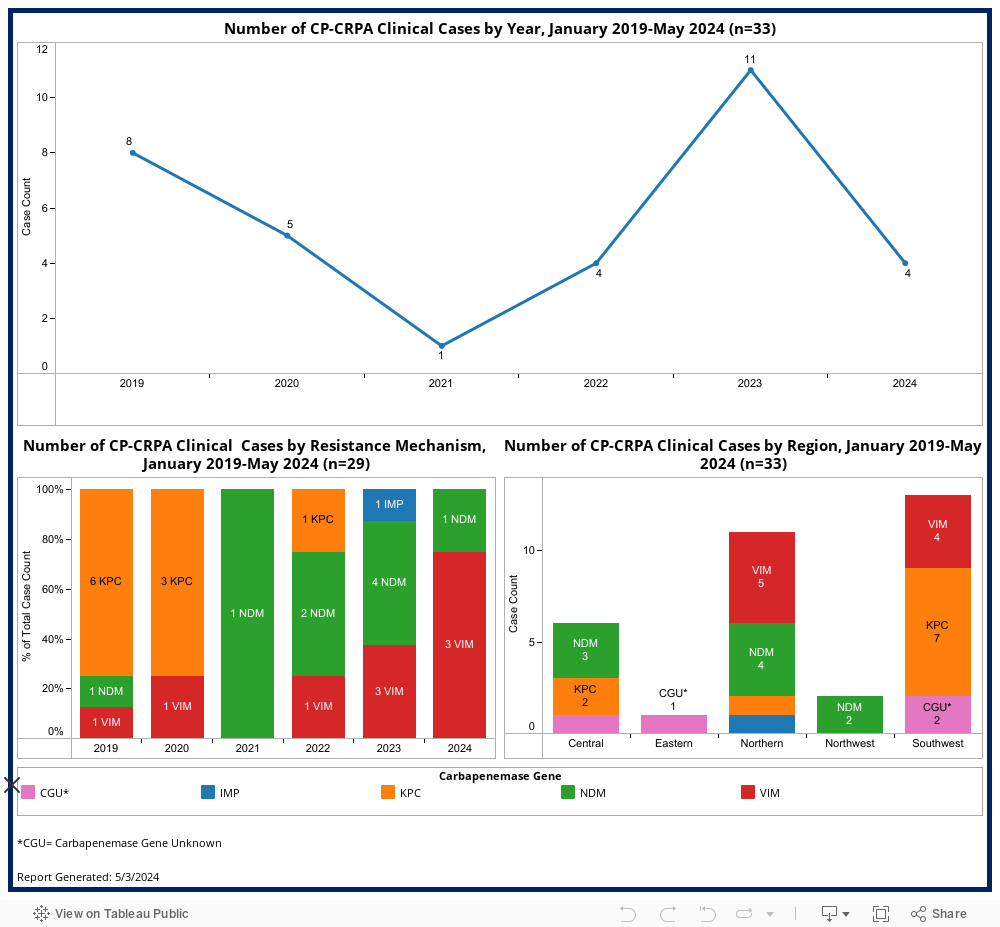
Carbapenemase-producing Carbapenem-resistant Pseudomonas aeruginosa (CP-CRPA)
According to the CDC’s AR Lab Network, less than 2% of carbapenem-resistant Pseudomonas aeruginosa (CRPA) isolates from the Mid-Atlantic region produced one of the five targeted carbapenemase genes. In addition to CP-CRPAs being reportable, laboratories are also required to forward CRPA isolates to the state public health lab where additional testing is performed to determine the presence of a carbapenemase and the specific gene target.
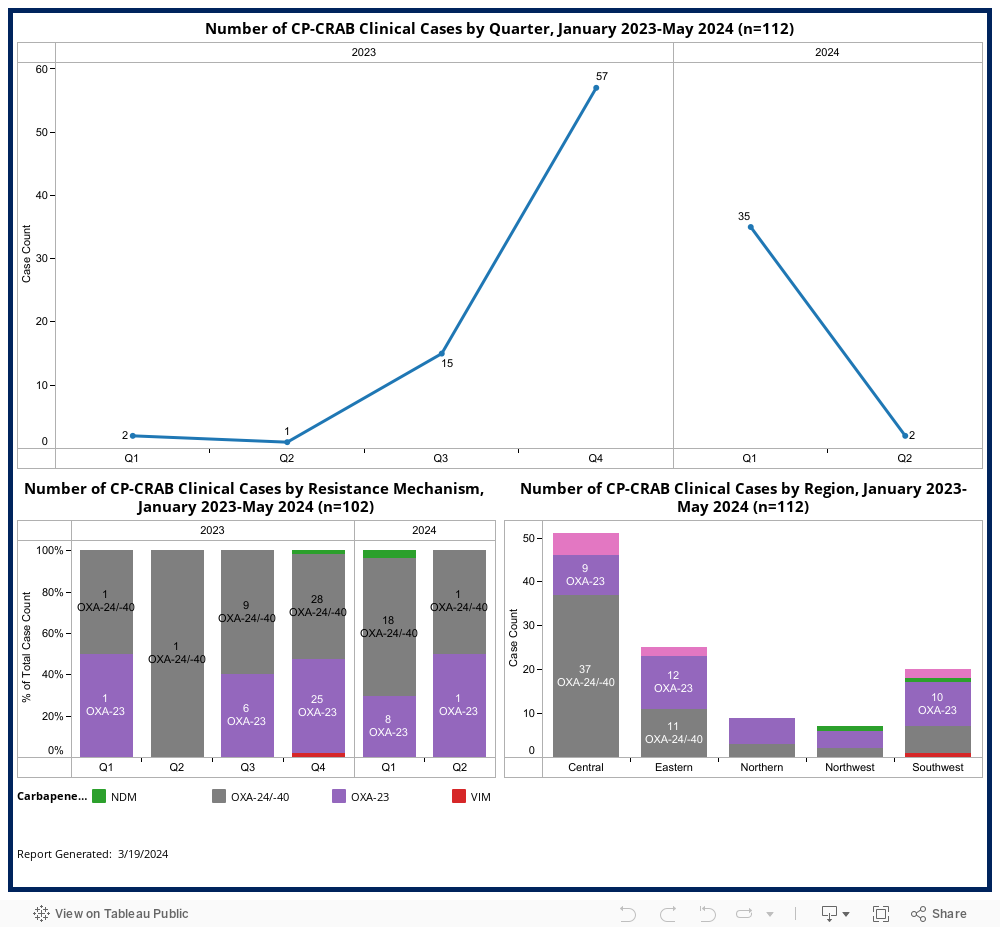
Carbapenemase-producing Carbapenem-resistant Acinetobacter baumannii (CP-CRAB)
Testing in the CDC’s AR Lab Network during 2019 found that carbapenemase genes were detected in 83% of Carbapenem-resistant Acinetobacter baumannii (CRAB) isolates tested. In Virginia, CP-CRAB is reportable, however laboratories are not required to forward CRAB isolates. Some laboratories voluntarily submit CRAB isolates to the public health laboratory for additional testing. Starting in 2023, DCLS implemented an expanded panel for CRAB carbapenemase testing. See additional information section for laboratory testing details. Data below are from select laboratories in Virginia and the data should be interpreted with caution as they may not be representative of every Virginia region.
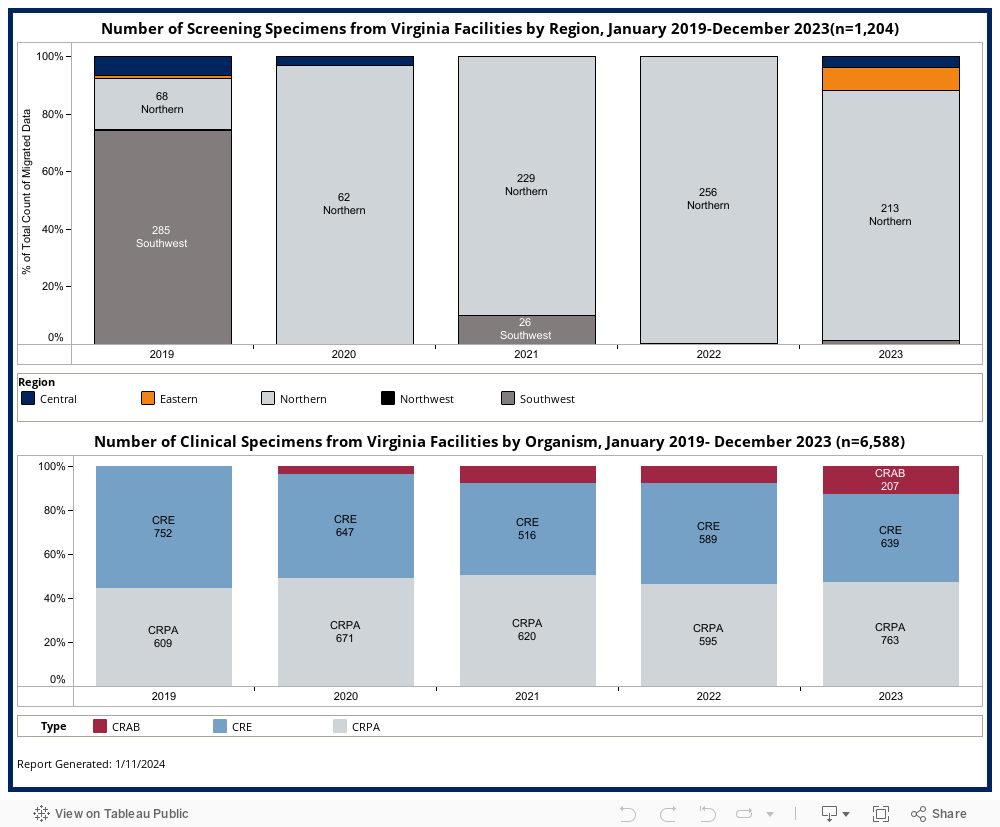
Laboratory Submissions
Lab submission data are included to aid in the interpretation of case counts. Number of screening specimens submitted for testing varies by region. Number of clinical specimens submitted varies by organism.
Additional Information
- How is a CPO case determined?
- Cases are determined using the CSTE Case Definition for CPOs. The CSTE case definitions were revised in January 2023. Cases counted prior to January 2023 were classified using the 2019 CSTE Case Definition.
- Where do the data come from?
- Healthcare facilities and/or clinical laboratories are required to report CPO cases to their local health department. Local epidemiologists determine case status and respond to cases by collecting data, providing infection prevention recommendations, and conducting a contact investigation. Laboratory and case information are entered in the Virginia Electronic Disease Surveillance System (VEDSS). The VDH Antimicrobial Resistance Epidemiologist queries VEDSS to develop these reports. Cases are assigned to a month based on the date the investigation was started at the local health department. Cases are assigned to a region of the state based on the local health department (LHD) investigator listed in VEDSS. LHD investigator is assigned (in most cases) by the location of the healthcare facility where the patient was seen at the time of specimen collection. Healthcare facilities can include acute care, long-term care, and outpatient facilities.
- How are laboratory data submitted?
- Virginia requires clinical laboratories to forward CRE and CRPA isolates to DCLS for additional testing to determine the presence of a carbapenemase. Clinical laboratories can also voluntarily send CRAB isolates for additional testing. Because CRAB isolate submission is voluntary, caution should be used when interpreting overall burden of carbapenemase-producing Acinetobacter baumannii in Virginia.
- What is the difference between screening and clinical cases?
- Screening cases are typically discovered during a screening process, such as admission screenings or if the patient was screened because of their contact with a known case. Specimens collected for screening are rectal swabs and are tested at the Mid-Atlantic Antimicrobial Resistant Laboratory Network. Screening specimens are only tested for the carbapenemase genes. Routine testing of screening specimens does not include organism identification, which is why the organism-specific tabs in this report do not include screening cases.
- Clinical cases can come from a variety of specimen sources (e.g., wound, urine, blood). These specimens may be submitted through our state public health lab (DCLS) or from other clinical laboratories.
- What testing is performed by the public health labs?
- Clinical specimens are forwarded to the Virginia Division for Consolidated Laboratory Services (DCLS) for additional testing. Testing varies by organism.
- Carbapenem-resistant Enterobacterales and carbapenem-resistant Pseudomonas aeruginosa testing is as follows:
- Phenotypic confirmation of carbapenemase production (mCIM)
- Molecular detection of resistance mechanisms by real-time PCR for mCIM positive isolates for the following targets (KPC, NDM, OXA-48, VIM, IMP)
- Carbapenem-resistant Acinetobacter baumannii testing is as follows:
- Molecular detection of resistance mechanisms by real-time PCR on all isolates for the following targets (IMP, KPC, NDM, OXA-23, OXA-24/40, OXA-48, OXA-58, OXA-235, and VIM)
- Carbapenem-resistant Enterobacterales and carbapenem-resistant Pseudomonas aeruginosa testing is as follows:
- Screening specimens are tested at the CDC’s Mid-Atlantic ARLN located in Maryland.
- Clinical specimens are forwarded to the Virginia Division for Consolidated Laboratory Services (DCLS) for additional testing. Testing varies by organism.