The Social Determinants of Health (SDOH) are a major determinant of population health outcomes. Depending on how they are measured and defined, the SDOH may account for up to 90% of the variation in health outcomes between communities. COVID-19 is no exception. Previous analysis examined how factors such as race and ethnicity, occupation, poverty and rurality, and housing are playing a role in COVID-19 outcomes in Virginia and elsewhere. Access to health resources is often a factor underlying health disparities, while increasing access can help alleviate disparities created by other factors. In the case of COVID-19, access to vaccines by at-risk populations is essential to addressing disparities. The post examines vaccine disparities by poverty, rurality, and SDOH at the census tract level in Virginia as of August 26, 2021.
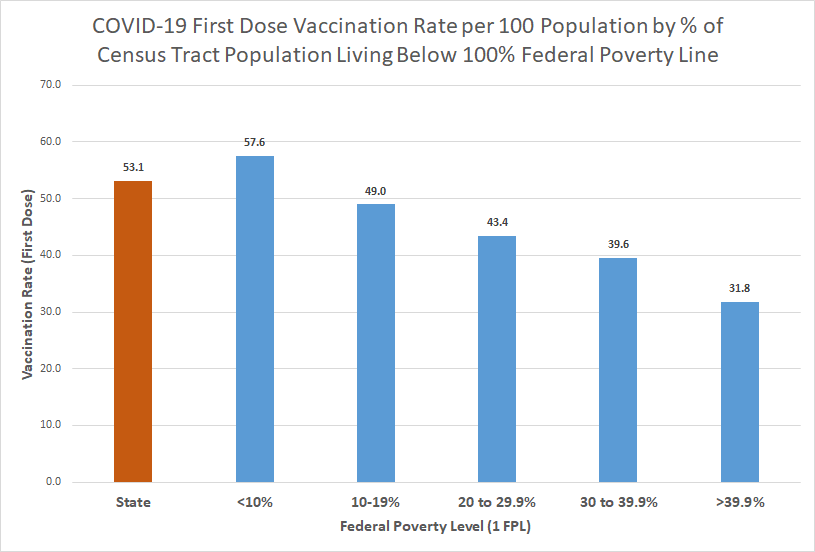
Poverty Level Disparities
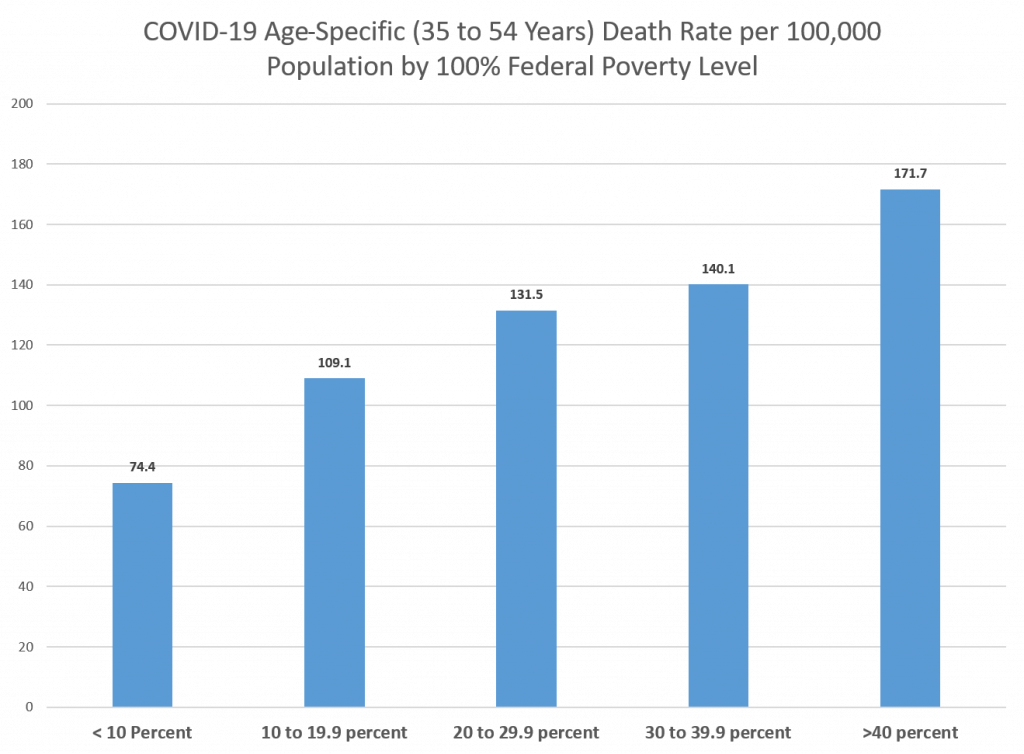
First Dose vaccination coverage varied widely by poverty level, with the highest coverage in those census tracts with less than 10% of the population living below 100% federal poverty level. However, the lowest coverage is found in census tracts with over 39.9% of the population living below 100% federal poverty level. One of the largest disparities in vaccination rates in Virginia is found among high and low census tract poverty levels.
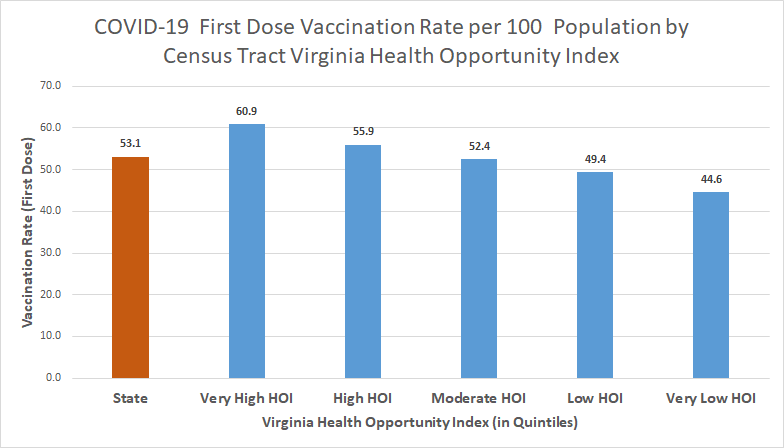
Health Opportunity Index Disparities
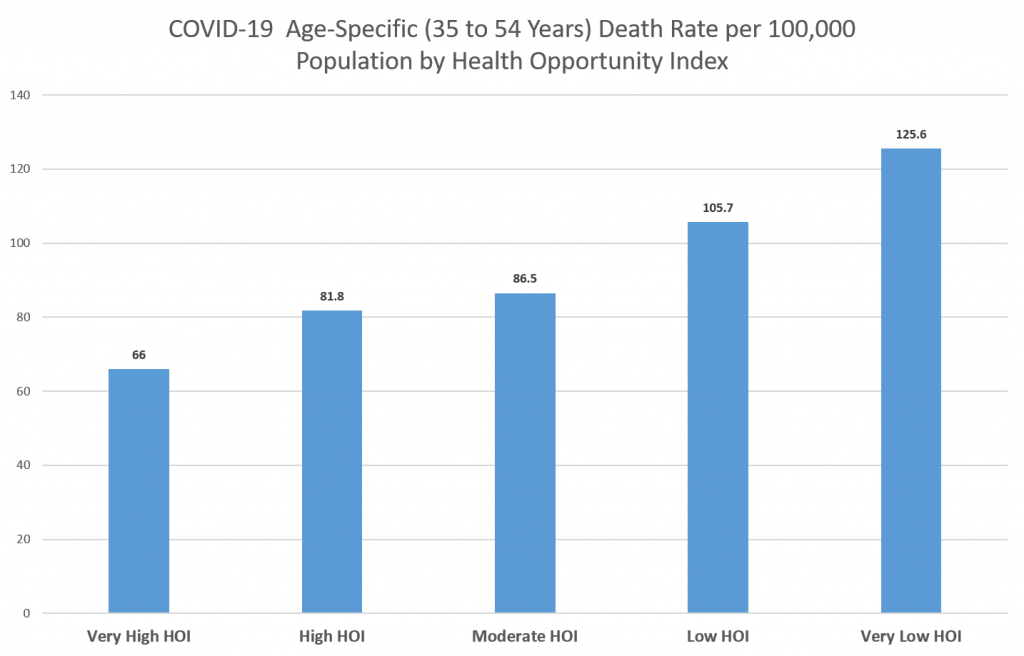
The Virginia Department of Health provides the Virginia Health Opportunity Index (HOI) which is a composite measure of the social determinants of health – the social, economic, educational and environmental factors that relate to a community’s well-being – at the census tract level. The index is divided into 5 levels – very high, high, moderate, low, and very low – and census tracts can be grouped into these 5 levels. Vaccination coverage was higher in high health opportunity census tracts than in low health opportunity census tracts. Persons living in the very high health opportunity census tracts were 37% more likely to be vaccinated as those in very low health opportunity census tracts.
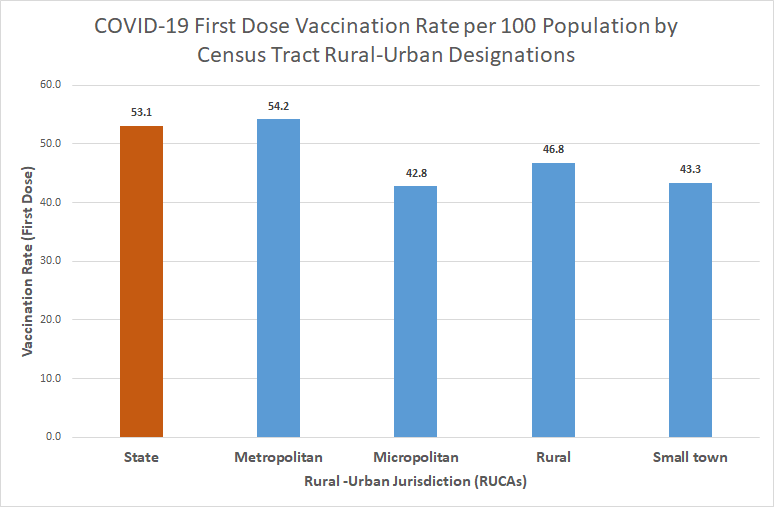
Rurality Disparities
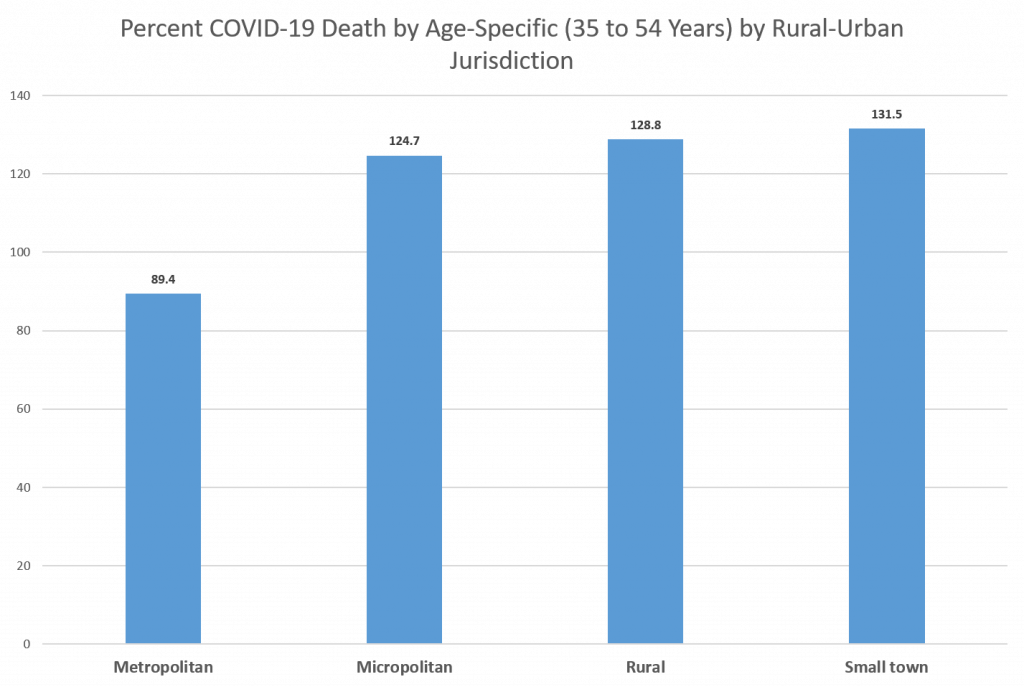
Rural and urban census tracts were classified by the Rural-Urban Commuting Area (RUCA) taxonomy and then further classified into groups – metropolitan, micropolitan, small town and rural. Based on the chart, it can be seen that, people living in metropolitan areas have a higher rate of COVID-19 first dose vaccination than those living in rural areas. People living in metropolitan areas are 16% more likely to have received their first vaccination than those in the rural areas.