
Last Updated: November 15, 2021
The Virginia Department of Health tracks COVID-19 disparities by race and ethnicity for cases, hospitalizations, deaths, and vaccinations. This is important because underlying health and social inequities put some racial and ethnic groups at greater risk than others. By examining disparities over the course of the pandemic, it is possible to get a sense of where they have improved and where improvement is still needed.
Early in the pandemic it became clear disparities were severe across the United States, so the Virginia Department of Health began tracking cases, deaths, and hospitalizations by race, ethnicity, age, and socioeconomic status, to learn how different groups were impacted. Mortality was disproportionately higher for racial and ethnic minority persons than for White persons.1 This analysis compares three different periods of the pandemic in Virginia to better understand disparities within the Commonwealth and how they have changed so far.
Health Disparity Rate Ratios
Rate ratios are used to quantify disparity. A rate ratio compares the rate of events in different groups to a reference group and expresses it as a simple ratio. A previous blog post, Health Disparity Rate Ratios, goes into greater detail about them. In general, higher rate ratios mean higher rates within one group compared to the reference group.
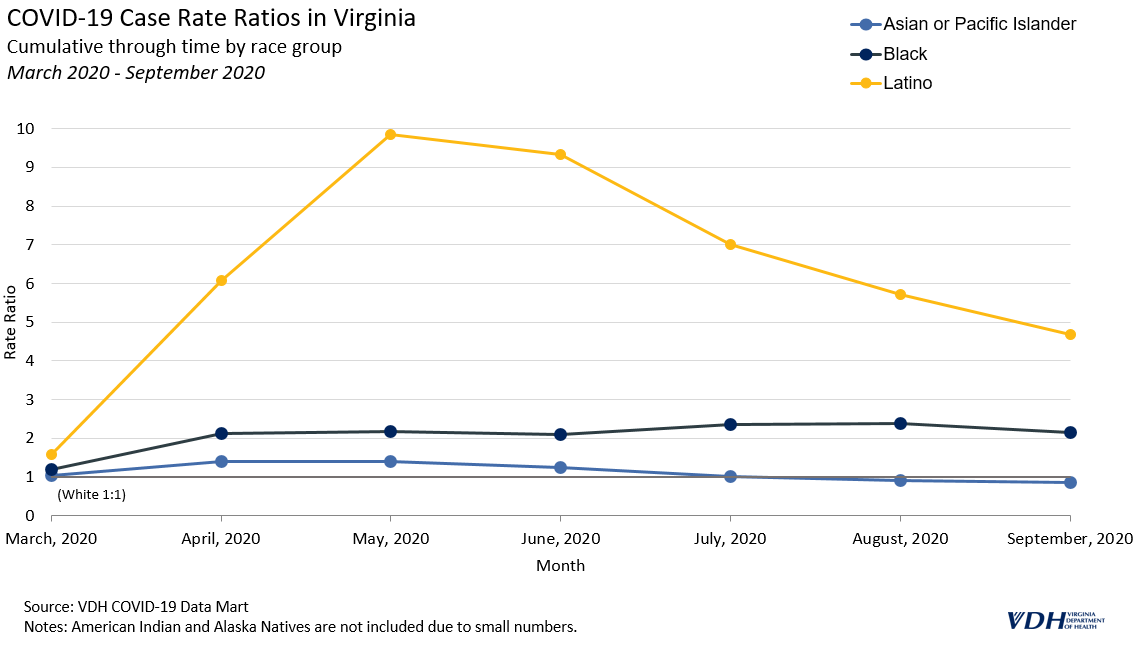
March 2020 – September 2020
During the spring and summer of 2020, cases surged across the United States and disparities were more pronounced than at any other point in the pandemic. The 7-day moving average of cases in Virginia hovered around 1,000 during this time. Latino people were most impacted initially; they were more likely to get COVID-19, and subsequently die from it, compared to any other group in Virginia, with case rates consistently at least five times the rate of White people. Black people also had case and death rates that were twice as high as White people.
Some of the early disparities in cases likely stemmed from outbreaks among front-line and essential workers, particularly those in the meat and poultry industry. Lessons learned from these early outbreaks helped to inform future responses and outreach. For example, one investigation into outbreaks in Chesterfield County and Richmond City identified lack of accessible health information in Spanish, lack of insurance and paid sick leave, and employment in frontline industries as risk factors for COVID-19 in Latino communities. Public health officials and policy-makers responded with strategies to address these disparities.
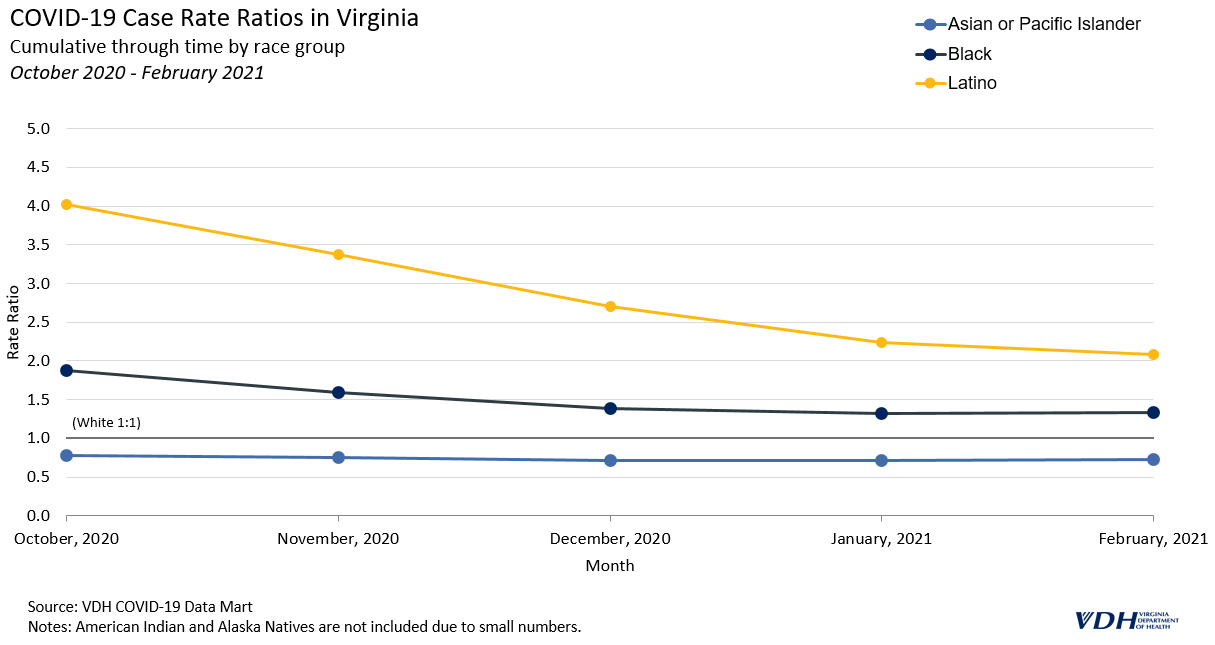
October 2020 – February 2021
In the fall of 2020 and winter of 2020-2021, the number of cases in Virginia reached new highs while racial and ethnic disparities began to decline. The 7-day moving average of cases rose from around 1,000 in October to over 5,000, and remained above 3,000 through February. This was the highest peak in cases during the pandemic so far.
During the peak, Latino people still had a case rate of about four times that of White people, but by January 2021, that number dropped to 2.2.
A similar trend can be seen for Black people, decreasing from 1.9 times that of White people to around 1.4 times. Asian or Pacific Islander people remained near or below the cumulative case rate of White people throughout the pandemic.
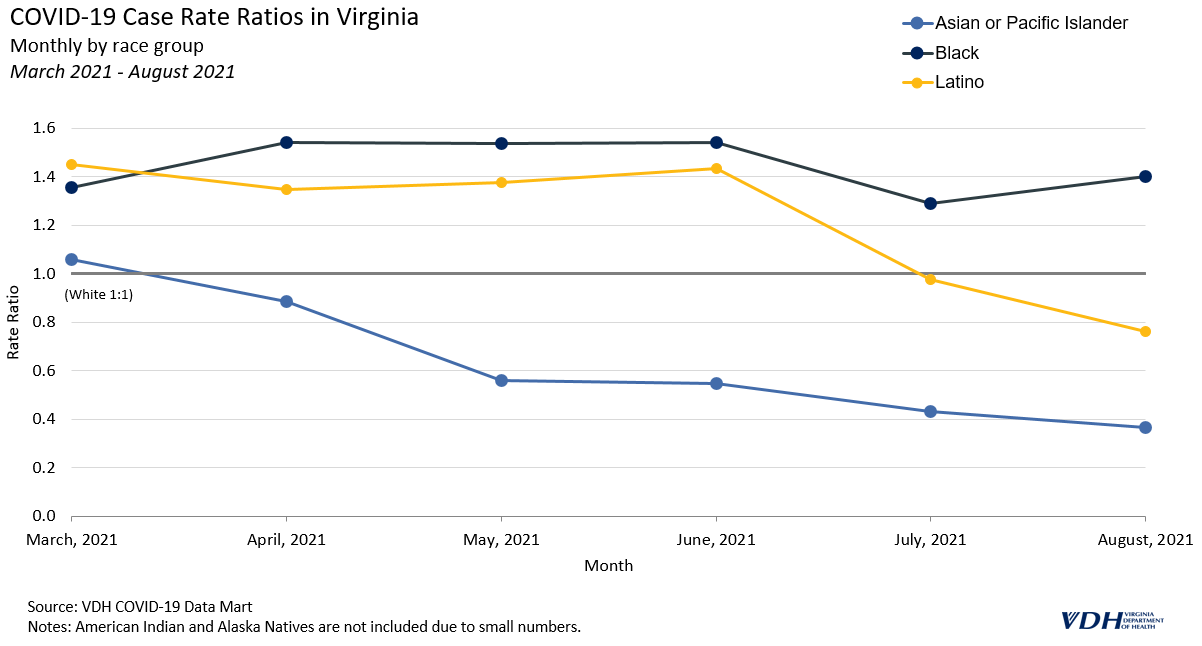
March 2021 – August 2021
Disparity in COVID-19 case and death rates changed significantly after March 2021, when 21% of people in Virginia had received at least one dose of vaccine and cases briefly dipped to lower levels. In June, the 7-day moving average was as low as 145, though it quickly returned to over 3,000. Now, with varying levels of vaccine uptake among racial and ethnic groups, COVID-19 disparities have shifted.
The current COVID-19 vaccines have been proven to be effective at preventing infection, severe illness, and death from COVID-19; they are the most important preventive measure to reduce the impact of the virus on individuals and communities. The extent to which racial and ethnic minorities are vaccinated has likely affected case and death rate disparities in Virginia.
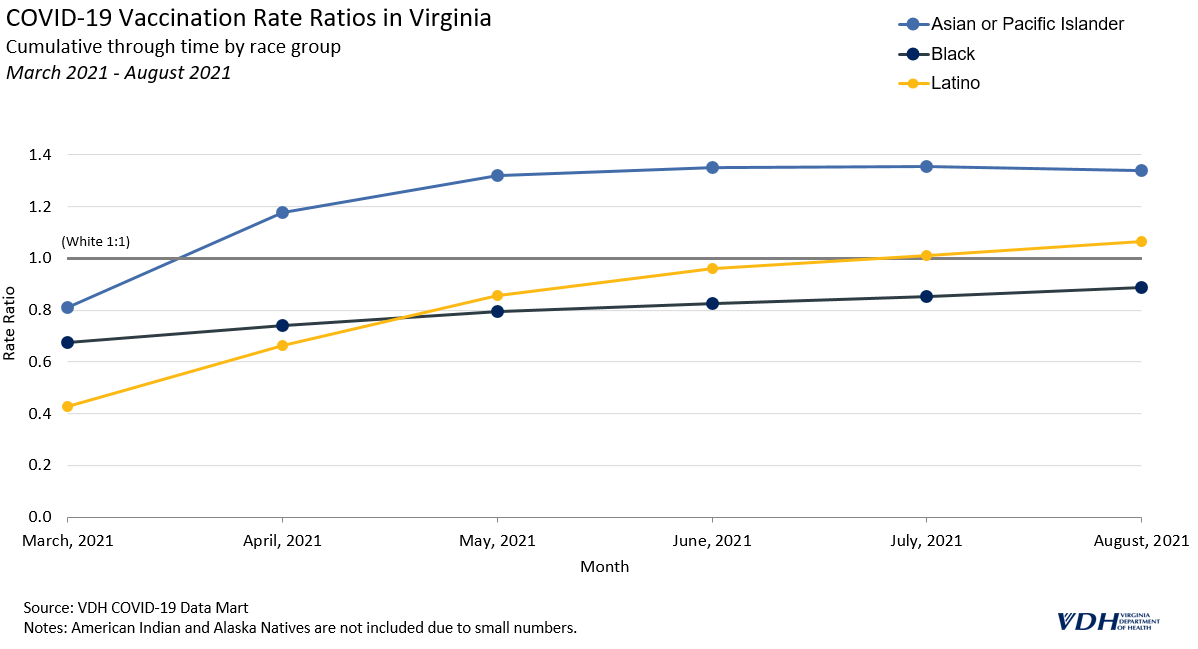
Asian and Pacific Islander people have a higher overall vaccination rate, around 1.3 times that of White people. Additionally, Latino people are now the second most vaccinated group, while White and Black people are less likely to be vaccinated.
Monthly rate ratios are better at indicating the direction of disparities, or current trend, than cumulative rate ratios. The following graph of monthly death rate ratios depicts a new trend from March 2021 onward, where case and death rate ratios for Latino people have better parity. Latino people had the highest death rates early in the pandemic.
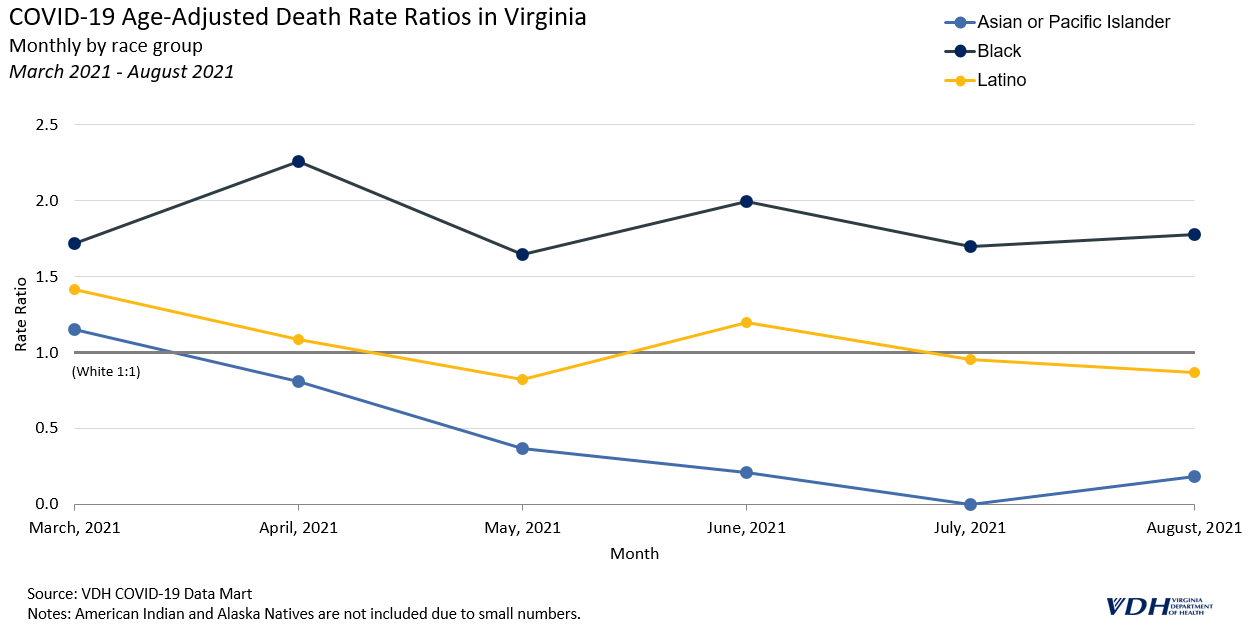
Vaccine hesitancy is a significant barrier to decreasing death rates for all groups in Virginia, and is a particular issue among Black communities. Further research is needed to fully understand the impact, but the extent to which different racial and ethnic groups in Virginia are getting vaccinated is likely affecting death rates from COVID-19. Trends in COVID-19 case and death rate disparities are likely to change as more people get vaccinated. The Virginia Department of Health updates rate ratios monthly on its COVID-19 Cases & Testing Dashboards to maintain its commitment to transparently tracking COVID-19 disparities in the Commonwealth.
__
* The impact of the Delta variant cannot be fully presented due to the lack of data points since July when it became the major variant.
*American Indian and Alaska Natives were not included in this analysis due to the small size of that population.
References
- Webb Hooper M, Nápoles AM, Pérez-Stable EJ. COVID-19 and Racial/Ethnic Disparities. JAMA. 2020;323(24):2466–2467. doi:10.1001/jama.2020.8598